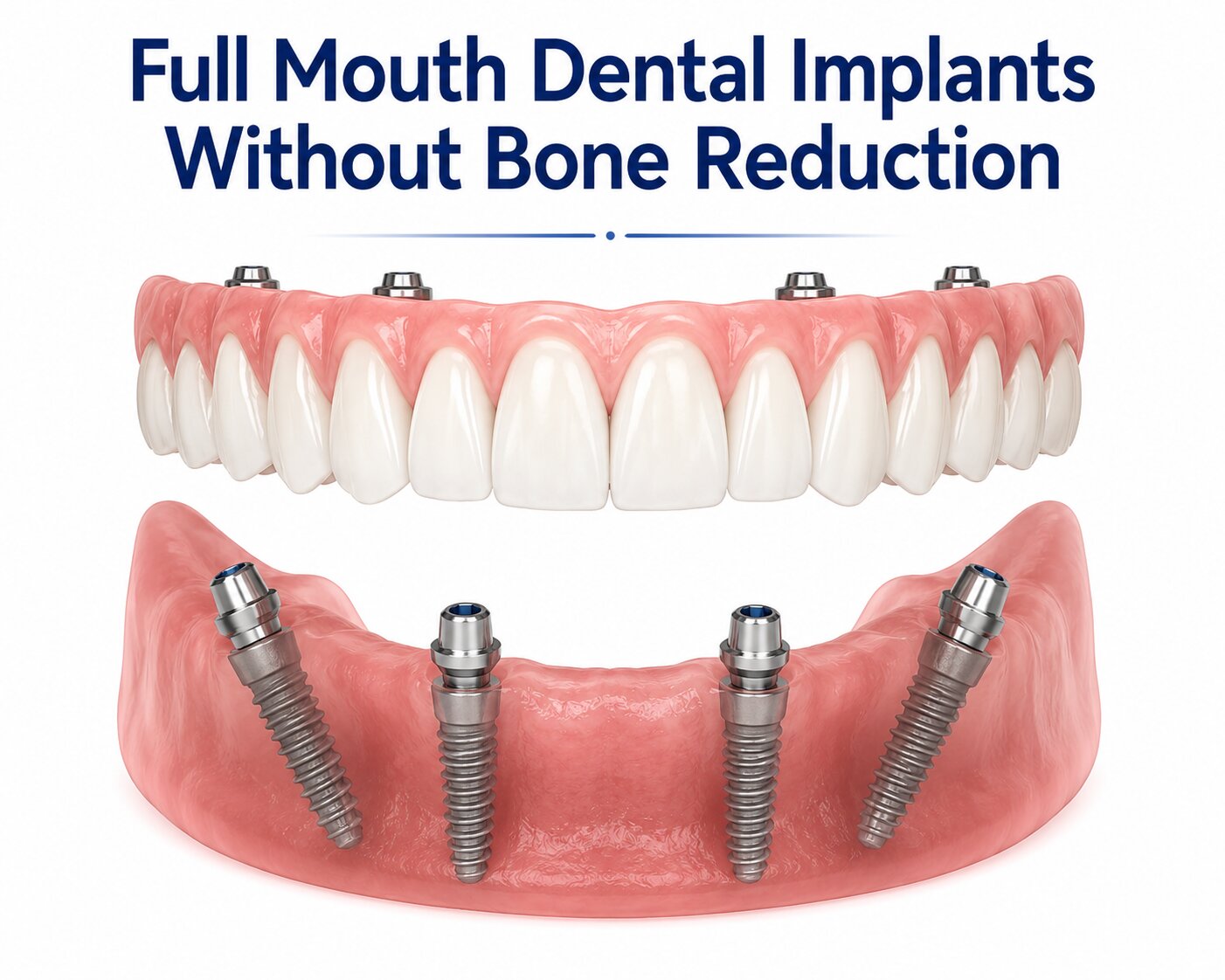
When you’re researching full mouth tooth replacement, you’ve likely come across terms like bone grafting, bone reduction, and sinus lifts. These procedures are sometimes necessary, but they’re not automatically required for every patient. The key question your implant dentist needs to answer first is whether your existing jawbone anatomy can support fixed teeth without surgical reshaping.
Full mouth dental implants without bone reduction are possible when your vertical restorative space, bone volume, and soft tissue anatomy are compatible with implant placement as-is. The goal in these cases is to design the fixed teeth around your natural structures rather than modify your anatomy to fit a standard prosthetic template.
Implant dentistry has advanced significantly. 3D imaging, angled implant placement strategies, and refined prosthetic planning now allow oral surgeons and implant dentists to work around natural anatomy more reliably than ever before. That said, not every patient qualifies, and knowing what factors determine candidacy can help you have a more productive conversation with your care team.
Key Takeaways
- Bone reduction is not always required for full mouth implants when adequate restorative space and bone volume are present.
- 3D imaging and precise implant placement design are central to planning a bone-preserving full arch case.
- Patients with significant bone loss still have options, including short implants, zygomatic implants, and graftless techniques.
When A Bone-Preserving Full Arch Approach Makes Sense
Preserving your existing jawbone architecture is often the preferred starting point in full arch planning. The anatomy that works in your favor includes adequate vertical restorative space, healthy gingival contours, and sufficient jawbone volume and density to support osseointegration (the process by which implants fuse with bone).
Adequate Vertical Restorative Space And Existing Anatomy
Vertical restorative space refers to the distance between your upper and lower jaws when biting together. There needs to be enough room to seat implant components and a prosthetic arch without the result looking or feeling overcrowded.
When bone resorption has occurred, the ridge may actually be positioned lower or higher than ideal, which can create more space than expected. In some cases, this means bone reduction is genuinely unnecessary because nature has already created the clearance your prosthetic requires.
Your implant dentist will evaluate your occlusal (bite) relationship, lip support, and smile line as part of this assessment.
Preserving Papilla And Gingival Contour
The papilla is the triangular soft tissue that fills the space between teeth. When you preserve it, your final result tends to look more natural and be easier to clean around. Reducing bone unnecessarily can compromise this tissue.
When gingival contour is intact and healthy, your surgeon has a cleaner canvas to work with. Preserving it avoids the need for later soft tissue grafting and supports long-term oral hygiene around implant prosthetics.
The esthetic outcome of fixed teeth often depends as much on what soft tissue is preserved as on the implants themselves.
How Jawbone Volume And Jawbone Density Affect Candidacy
Jawbone volume and jawbone density are evaluated separately but are both essential. Volume refers to how much bone is present in three dimensions. Density refers to the quality and hardness of that bone, which affects how well osseointegration proceeds.
Insufficient bone density, particularly in the upper jaw, can slow or compromise healing. Upper jaw bone loss is common after prolonged denture wear or tooth loss, and the upper jaw bone tends to be naturally less dense than the lower jaw.
Patients with adequate volume but low density may still be candidates for a bone-preserving approach, though implant number and angulation strategies are adjusted accordingly.
Treatment Planning And Implant Placement

Careful planning is what makes it possible to place implants without altering your bone. Angled implant placement, prosthetic design, and advanced imaging all work together to create a result that fits your anatomy rather than forcing your anatomy to fit a generic plan.
The Role Of 3D Imaging And CT Scans
CT scans (cone beam computed tomography) give your implant dentist or oral surgeon a precise three-dimensional view of your jawbone, sinuses, nerve canals, and available bone dimensions. This is not optional in full arch cases; it is the foundation of safe planning.
3D imaging allows your care team to map exactly where implants can be placed, at what angles, and at what depths without risking nearby structures. It also identifies areas of bone loss or low density before surgery, reducing surprises during the procedure.
When a bone-preserving approach is being considered, CT scans help confirm that sufficient bone volume exists at each planned implant site.
How Implant Placement Is Designed Around Natural Structures
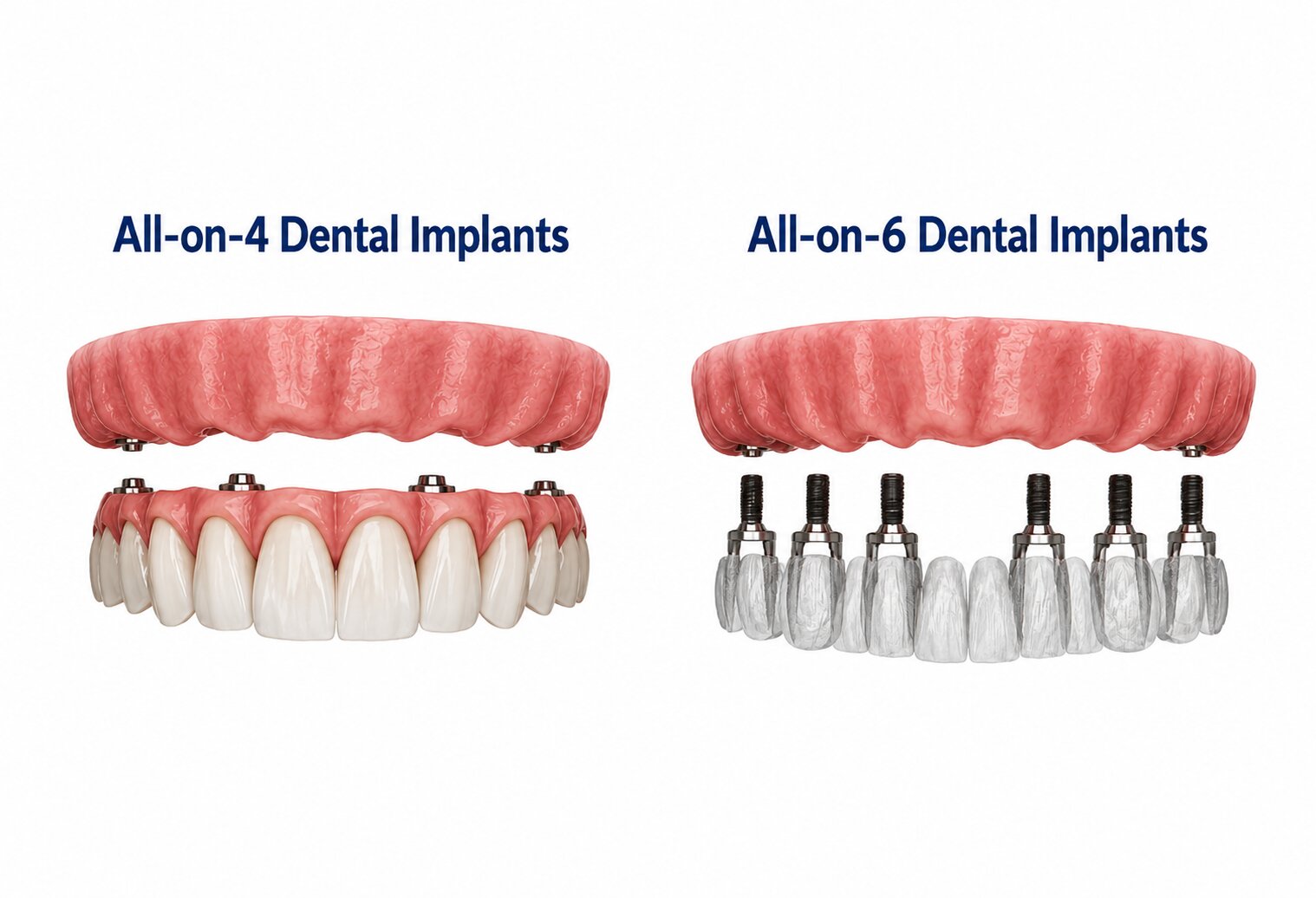
Rather than reshaping bone to accommodate straight implants, angled implant placement allows the surgeon to direct implants into denser or wider regions of available bone. This is central to the All-on-4 and All-on-6 concepts, where posterior implants are tilted to engage more bone and avoid anatomical structures like the sinuses or inferior alveolar nerve.
Angled implants can reach bone that would otherwise require grafting if only vertical placement were used. The prosthetic components are then designed to compensate for the angulation, resulting in a fixed arch that looks and functions normally.
This design-first approach means the prosthetic is planned before surgery, not after.
Immediate Loading And Full-Arch Prosthetic Planning
Immediate loading means a temporary fixed prosthetic is attached to implants on the same day as surgery, or within a few days. This approach is well-documented in full arch cases and is often used when implants achieve adequate initial stability at placement.
Not every patient is a candidate for immediate loading. Bone density, implant position, and your overall health all factor into this decision. When it is appropriate, it avoids weeks of wearing a removable provisional and gives you functional fixed teeth during the healing period.
Your prosthetic arch is typically pre-designed using digital planning before your surgery date, which improves fit and reduces chair time.
Alternatives When Anatomy Or Bone Is Limited

Not every patient has the bone volume or density to support a standard full arch approach, and that does not mean implants are off the table. A range of alternative implant techniques and graftless strategies exist for patients where the available anatomy requires a different plan.
Dental Implants Without Bone Graft In Selected Cases
Dental implants without bone grafting are possible when residual bone is in the right location and of adequate quality, even if total volume seems limited. The “no bone graft” approach relies on selecting implant sizes, angles, and positions that work within what exists.
Ridge expansion methods are one option for narrow bone ridges. Rather than adding graft material, the existing ridge is gently widened using specialized instruments, and implants are placed simultaneously or shortly after. Socket preservation (placing graft material at extraction time) can also reduce the need for later bone grafting by maintaining ridge width before implant placement.
For patients who want dental implants without bone graft whenever possible, a thorough CT scan evaluation is the starting point to see what anatomy is genuinely available.
Short And Mini Options For Reduced Bone Height Or Width
Short dental implants (typically under 8 mm) are designed for situations where bone height is limited, such as below the sinus floor in the upper jaw or above the nerve in the lower jaw. Research supports their use in appropriate cases, and they can eliminate the need for sinus lifts or bone grafting procedures in selected patients.
Mini dental implants have a smaller diameter and are sometimes used to stabilize full arches when standard implants are not feasible due to narrow bone width. Mini implants carry different load-bearing considerations and are not always appropriate for full fixed arches; your provider should explain the specific tradeoffs for your case.
Short and mini options are not universally interchangeable with standard implants but represent genuine solutions when bone dimensions are the limiting factor.
Advanced Graftless Solutions For Severe Maxillary Deficiency
When upper jaw bone loss is severe, zygomatic implants offer a well-studied alternative. These longer implants anchor into the zygomatic bone (cheekbone) rather than the maxilla, bypassing the need for sinus lifts entirely. They are typically placed by oral surgeons with specific training in this technique.
Pterygoid implants are another sinus lift alternative, placed into the pterygoid process at the back of the upper jaw. They provide posterior support in the maxilla without entering the sinus, making them useful in certain bone patterns.
Both zygomatic and pterygoid implants are considered advanced alternative implant techniques. They are not appropriate for every provider or every patient, but they represent meaningful options for those who have been told conventional implants are impossible due to upper jaw bone loss.
Benefits, Risks, And Long-Term Decision Factors
Whether you preserve bone or require grafting, full arch implants represent a significant long-term commitment. The decisions made during planning directly affect esthetics, hygiene access, and how the implants perform over years of use.
Esthetics, Function, And Oral Hygiene Considerations
Fixed teeth that are designed around your natural anatomy tend to produce more lifelike esthetic results. Preserved papilla, natural gingival contour, and appropriate restorative space all contribute to a prosthetic that looks proportionate and integrates well with your face.
Oral hygiene around full arch implants requires consistent effort regardless of surgical approach. Water flossers, interdental brushes, and regular professional cleanings are essential. Prosthetic design affects how easily you can clean underneath the arch; your dentist should show you how to maintain access before your final prosthetic is delivered.
Function, including bite force and speech, is generally well-restored with fixed implant arches when planning is thorough and occlusion is properly managed.
Implant Success Rates, Failure Risks, And Nerve Safety
Implant success rates for full arch cases are high in well-selected patients, with most studies reporting cumulative survival rates above 95% over five to ten years. That said, implant failure does occur, most often due to bone loss around the implant (peri-implantitis), infection, or poor osseointegration.
Smoking, uncontrolled diabetes, and poor oral hygiene significantly affect implant success factors. Nerve damage is a recognized risk, particularly in the lower jaw where the inferior alveolar nerve runs close to implant sites. CT scan-based planning substantially reduces this risk when performed carefully.
Implant failure due to progressive bone loss after placement is distinct from initial failure; long-term maintenance and regular imaging help catch early signs before they become serious.
Comparing Full-Arch Implants With Other Tooth Replacement Options
In a dental implant vs bridge comparison, full arch implants avoid the need to use remaining natural teeth as anchors, which can weaken those teeth over time. Implants also help maintain bone by providing stimulation that a bridge or denture cannot replicate.
Tooth replacement options like removable full dentures require no surgery but come with ongoing fit problems, bone loss acceleration, and reduced chewing efficiency compared to fixed implants. The tradeoff is lower upfront cost and less surgical risk.
Implant-supported overdentures offer a middle path: implants anchor a removable prosthetic, which improves stability over conventional dentures while being less complex than a fully fixed arch. These may suit patients who are not ideal candidates for fixed solutions.
Frequently Asked Questions
What options are available for full-arch tooth replacement if there isn’t enough jawbone for conventional implants?
When standard implant placement is not possible due to bone volume limitations, options include short implants, mini implants, zygomatic implants, pterygoid implants, and ridge expansion methods. Bone grafting procedures can also rebuild volume over time, though they add treatment length and recovery. A CT scan evaluation is essential to determine which path fits your specific anatomy.
How do zygomatic implants compare to traditional implants for patients with severe upper jaw bone loss?
Zygomatic implants anchor into the cheekbone rather than the upper jawbone, which makes them useful when the maxilla lacks sufficient volume for standard implants. They avoid sinus lifts entirely and can support a fixed full arch. They require specialized surgical training and are not as widely available as traditional implants, so finding a qualified provider matters.
Are pterygoid implants a reliable alternative for avoiding sinus lifts or bone grafting in the upper jaw?
Pterygoid implants engage dense bone at the back of the upper jaw and provide reliable posterior support in selected patients. Published studies report good long-term success in carefully chosen cases. They are typically used in combination with anterior implants rather than as a standalone solution for the full arch.
What are the typical costs for full-mouth implant solutions when significant bone loss is present?
Full mouth implant treatment with significant bone loss typically costs more due to additional procedures like grafting, zygomatic implants, or sinus lifts. In the US, full arch implant cases can range from roughly $20,000 to $50,000 or more per arch depending on complexity, the provider’s expertise, and what supplementary procedures are required. Getting a detailed itemized treatment plan from your provider is the most reliable way to understand your specific costs.
Why do dental implants fail due to bone loss, and how can that risk be reduced in a full-arch case?
Peri-implantitis, an infection that causes progressive bone loss around an implant, is one of the leading causes of late implant failure. Consistent oral hygiene, regular professional maintenance, and prosthetic designs that allow cleaning access significantly reduce this risk. Patients who smoke or have uncontrolled systemic conditions face elevated failure risk and should address those factors before or during treatment.
How do mini implants compare to standard implants for stabilizing a full set of teeth in low-bone situations?
Mini implants have a smaller diameter and can be placed in narrower ridges where standard implants would not fit. They are more commonly used to stabilize removable overdentures than fully fixed arches, due to their lower load-bearing capacity. In the right clinical scenario with appropriate prosthetic design, they can provide meaningful support, but your provider should be transparent about the limitations compared to standard diameter implants.



